Hernia Surgery in Delhi
Robotic or Laparoscopic
SURGERY METHOD
2 weeks
RECOVERY TIME
1-2 hours
TIME UNDER SURGERY
Internal organs in the abdominal cavity are covered by protective layer of muscle and connective tissue known as fascia. Any weak spot in the muscle can rupture through which the content inside the abdominal cavity like intestine or fatty tissues can protrude outward and develop hernia.
A hernia can be caused by weakness of the abdominal wall, any incision or scar or congenital predispositions. The defect cannot be treated by medical management. Surgical intervention is required to treat hernia. A reducible hernia is one which can be pushed back into the opening.
All hernia should be treated on time regardless of small and asymptomatic hernia. After examination surgeon can identify the characteristics of hernia that may produce high risk of developing problem such as incarnation or strangulation. Sometimes the hernia neck opening in the muscle is quite small and hernia sac is large, this can create emergency situation if hernia sac gets trapped in the small neck opening
Hernia Classifications
Inguinal Hernia
Femoral Hernia
Ventral Hernia
Umbilical Hernia
Paraumbilical Hernia
Hiatus Hernia
Spigelian Hernia
Lumbar Hernia
1. Inguinal Hernia: Inguinal hernia or Groin hernia is estimated to be 27 to 43 percent in males and 3 to 6 percent in females. Inguinal hernias are more common in men. Inguinal hernia occurs when abdominal tissues or intestines bulge out through a weak spot in the muscle of the abdominal wall around the groin area. In men, the spermatic cord pierces the muscle, and in females, the round ligament pierces the muscle. Inguinal hernia can be bilateral or single-side. Patients often seek the expertise of specialists for inguinal hernia surgery in Delhi.
Direct Inguinal Hernia: A Hernia sac can penetrate through the wall of the inguinal canal due to Increased intra-abdominal pressure or cough or straining can cause direct inguinal hernia
Indirect Inguinal Hernia: This kind of hernia is congenital, Inguinal Canal fails to close before birth and abdominal contents protrude through the internal inguinal ring into the inguinal canal and may extend into the scrotum in the male or extend into the skin fold at the vaginal opening in the females
As Compared to inguinal hernia, femoral hernia cases are fewer, accounting for approx. 3% of total groin hernias. The incidence of femoral hernia is 10 times higher in females than males. A femoral hernia develops when the abdominal contents pass through a weak spot known as the femoral canal, often during pregnancy or childbirth. The bulge or hernia sac in a femoral hernia appears near the groin, upper thigh, or skin folds surrounding the vaginal opening. Femoral hernias should be repaired urgently due to a high risk of strangulation. For such cases, patients often consult a hernia surgery specialist in Delhi.
Ventral Hernia occurs when the intestine or abdominal tissues protrude through a weak ventral muscle at any location on the abdominal wall.
Three common types of ventral hernia are:
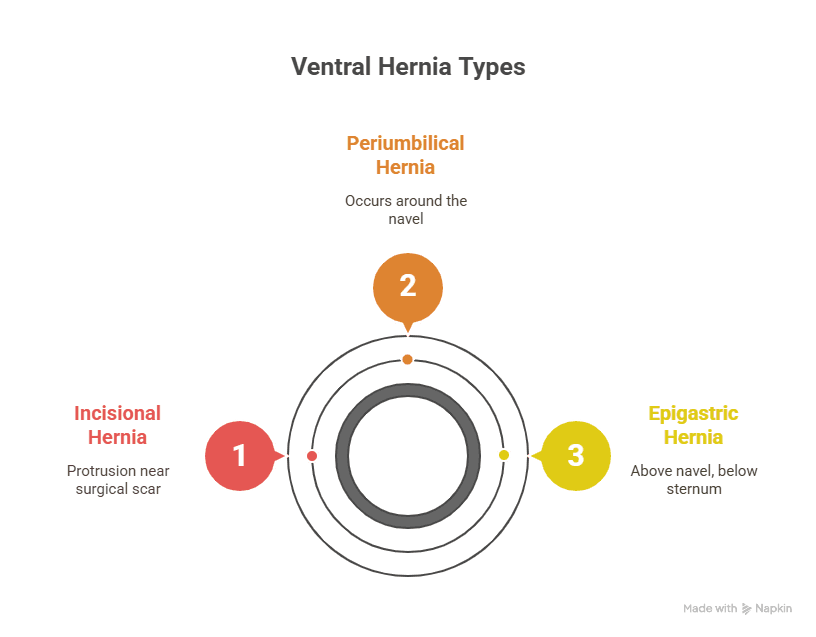
Incisional Hernia: An abnormal protrusion along or close to the surgical scar
Periumbilical Hernia: Occurs around the navel area
Epigastric Hernia: Occurs in the epigastric region above the belly button and below the sternum
Umbilical Hernia: Protrusion of bowel content through a defect near the belly button. Dr. Aloy Mukherjee is frequently consulted for umbilical hernia surgery in Delhi.
Hiatus Hernia: Occurs when the stomach bulges into the chest through the opening or weakness of the diaphragm muscle. For patients needing the best hiatal hernia surgery in Delhi, laparoscopic methods offer superior outcomes.
Irrespective of the site hernia can be classified into following:
Reducible Hernia: When the lump or bulge can be gently reverse or push back to original place through the opening of weak muscle known as reducible hernia
Irreducible Hernia: When the content of the hernia cannot be pushed back in the abdomen is known as irreversible hernia
Incarcerated hernia: In this hernia bulge cannot be pushed back and intestine or tissue trapped in the hernia sac and can cause obstruction
Strangulated Hernia: A hernia is strangulated if the intestine is trapped in the hernia pouch and the blood supply to the intestine is decreased due to compromised blood supply. This is a surgical emergency.
Causes of Hernia
Increased abdominal pressure is the most important factor for developing hernia. It could be because of pregnancy, ascites, cough, COPD straining.

The most common causes of hernias in adults are:
Pre-existing weakness of the abdominal wall
Straining such as during child birth or weight lifting
Chronic constipation
Obesity
COPD
Enlarged prostate (Straining during urination)
Chemotherapy drugs and corticosteroids
Surgical site infection
Repetitive vomiting
Increased intra-abdominal pressure
Pregnancy
Signs and symptoms
A protrusion or bulge in the abdominal wall or groin area, increases during physical activity and decreases while lying down
Dull ache or Pain in the protruded area (worse with activities)
Vomiting and constipation
Symptoms of a strangulated hernia
Abdominal distension, tenderness, and pain
Discoloration of the skin around protruded area
Vomiting
Constipation
Diagnosis
The primary diagnosis of any hernia is clinical examination. The bulge become more prominent while coughing .90 % of hernia can be diagnosed through physical examination.
Ultrasound
MRI or CT scan
These imaging test confirm the size of the defect and determine nature of the contents of the hernia
Treatment of Hernia
All hernias should be repaired however if the hernia is small and asymptomatic sometimes that hernia can be watched regardless it’s a good idea to consult a specialist if you have been diagnosed with hernia because specialist or hernia surgeon will be able to examine and identify the characteristics of the hernia that may put you a higher risk of developing problems such as incarnations or strangulations (Sometimes hernia neck or opening in the muscle is quite small but the hernia sac or the contents that protrude into can be rather large, so in that instance incarnation or strangulation can occur ). In such situations, Patients often look for the best doctor for hernia surgery in Delhi to avoid risks like strangulation. Early intervention is simpler; delayed treatment increases surgical complexity.
Medical management of hernia treatment is not available. Once the defect occurs surgery is the only treatment choice.
Advanced Hernia Surgery in Apollo Delhi can avoid the complications due to hernia defects. Delaying the hernia surgery can increases the defect, smaller hernia surgery is less complex while bigger hernia increases the complexity of surgery and increases the recovery time.
In some cases, delayed hernia surgery can become life-threatening and require emergency surgery like strangulated hernia
The Goal of Hernia Surgery
The goal of fixing a hernia is to less damage to tissue as possible to get the best possible result
The patient can resume day-to-day work very soon
Important steps in the Hernia Surgery
1st Step is to reduce the content back into the abdominal cavity
The second step is to repair the hole by sutures
3rd step is to reinforce the repair by putting the mesh. By putting the mesh recurrence rates are much lower
Surgical Approach for Hernia Surgery
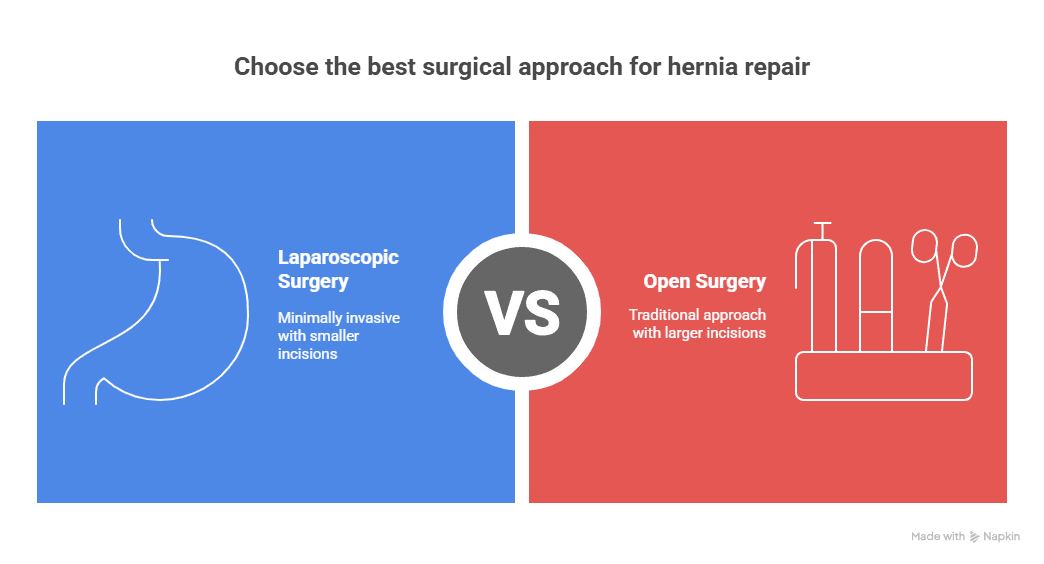
1. Laparoscopic Hernia Surgery:
Laparoscopic Hernia Surgery is a surgical procedure used to repair hernias. In laparoscopic hernia surgery through small incisions, trocars are inserted into the abdomen. A camera is inserted through the trocar to see the magnifying view of hernial contents (omentum or intestine) on a monitor and the surgeon can start surgery to reduce the defects, finally, hernia defects is fixed with non-absorbable sutures and adequately sized mesh,
Advantages of Laparoscopic Hernia Surgery
Hernia defects can be fixed with small incisions, patient experiences less pain, faster recovery, early healing, and small scars.
In laparoscopic hernia surgery, the laparoscope magnifies the internal view, this gives a better view to the surgeon compared to open surgery.
In laparoscopic hernia surgery there is less manipulation of tissues, so patients will experience less pain..
Laparoscopic hernia surgery can help the patient to be discharged early and a patient can resume normal activities within a very short period
Open Hernia Surgery
Open hernia surgery is traditional techniques for repairing hernias. It involves making a single, longer incision over the site of the hernia to access the protruding tissues and repair the muscle defect. While laparoscopic procedures are increasingly popular, open hernia surgery in Delhi remains an essential and reliable option, especially for large, recurrent, or complex hernias.
Which technique is the best for hernia?
The reconstructive options for hernia repair are diverse and must be tailored to a given clinical condition
The best technique for hernia repair depends upon:
Patient factor, Hernia Factor, Location of hernia, Size, and complexity
Patient comorbidities, hernia characteristics, and skin/soft tissue factors will impact the technique chosen for the repair
Technique of Hernia Surgery:

Fundamentally, there are three different techniques for repairing a hernia with mesh. The method chosen by the best hernia surgeon in Delhi typically depends on the particular condition of the patient undergoing hernia surgery. The following are the standard surgical techniques used in hernia mesh surgeries
Transabdominal pre-peritoneal or TAPP Technique
In this technique, the surgeons enter the peritoneum, i.e. the thin innermost membrane of the abdominal wall. They then place the surgical mesh in the appropriate layer of the abdominal wall with a small incision, so that it does not come in contact with the internal organs.
Totally Extra-peritoneal or TEP Technique
In this type of surgery, the surgeon essentially avoids the peritoneal cavity. The TEP surgery is typically more complicated to perform than the TAPP surgery, but it also involves the use of surgical mesh. Surgeons usually opt for this procedure because it results in fewer complications as compared to TAPP surgery.
Intraperitoneal On-lay Mesh Technique or IPOM Technique
In this technique, the surgeon enters the peritoneal cavity to implant a mesh on the inside of the peritoneum. The implanted surgical mesh comes in contact with the intestines and the other organs. The IPOM technique became popular in the 1990s and is typically much easier and faster to perform as compared to both, TAPP and TEP.
Complex Hernia:
A complex hernia refers to a hernia that is either very large in size or located in a challenging anatomical region, such as near the ribs or hip bones. These hernias often present greater surgical difficulty and are commonly associated with failed previous hernia surgeries, making them more complicated to treat. Patients often seek consultation with the best hernia surgeon in Delhi NCR for safe and effective management of such cases.
Complex hernias may also arise in individuals with underlying connective tissue disorders or risk factors such as obesity, diabetes, smoking, or prolonged steroid use. These conditions weaken the abdominal wall and predispose patients to primary hernia formation, leading many to consider expert evaluation from the best doctor for hernia surgery in Delhi.
Characteristics of Complex Hernia:
Hernia defect is greater than 8cm
Loss of abdominal domain
Fistulas, history of mesh infection
History of prior hernia repair, multiple failed repairs
History of prior open surgery
Body mass index (BMI) >35
High-risk medical conditions including diabetes, obesity and smoking
The most important for developing complex hernia is Incisional Hernia
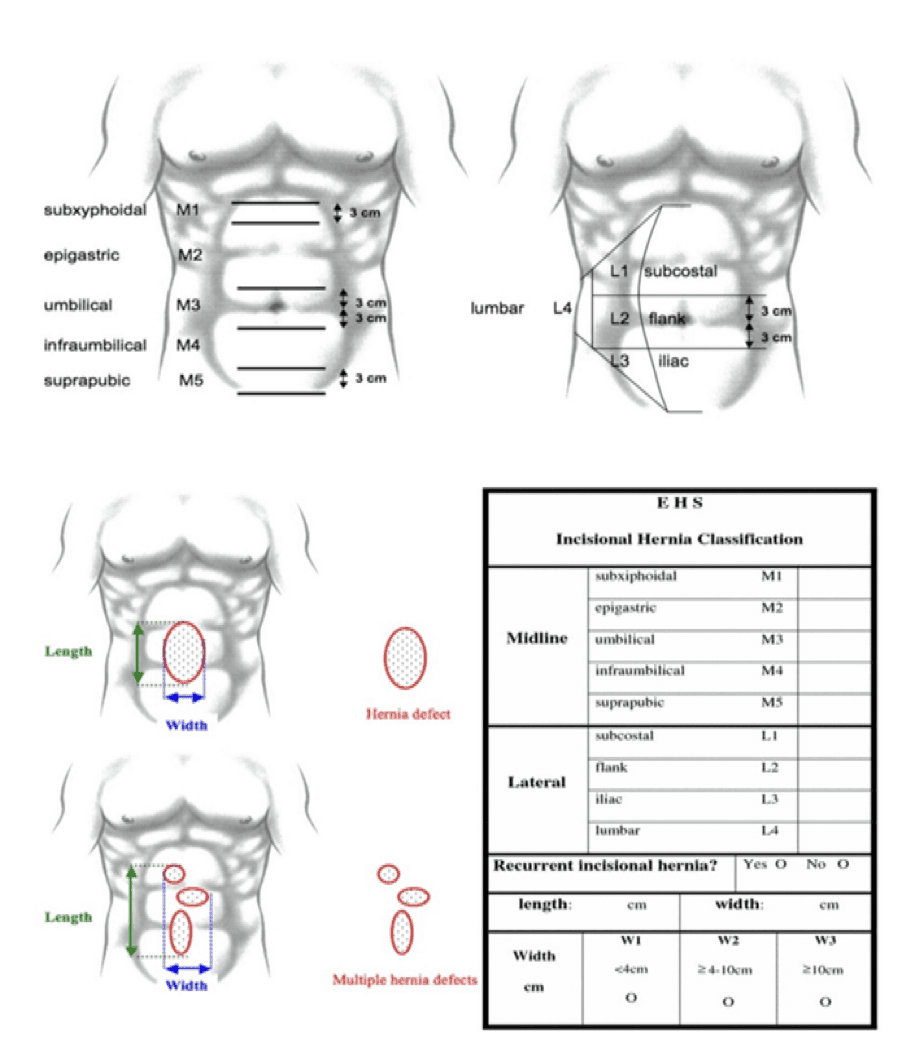
Incisional Hernia:
Incisional Hernia occurs in people who have had prior operation. The site of incision or scar of previous surgery can cause an area of weakness, as scar tissues never as strong as native tissue and that area of weakness causes a tear in the abdominal which creates a hole. In the presence of increased intra-abdominal pressure and potential risk factors (such as smoking or obesity), the contents of the abdomen push through creating a bulge known as incisional hernia.
Risk Factors for Incisional Hernia:
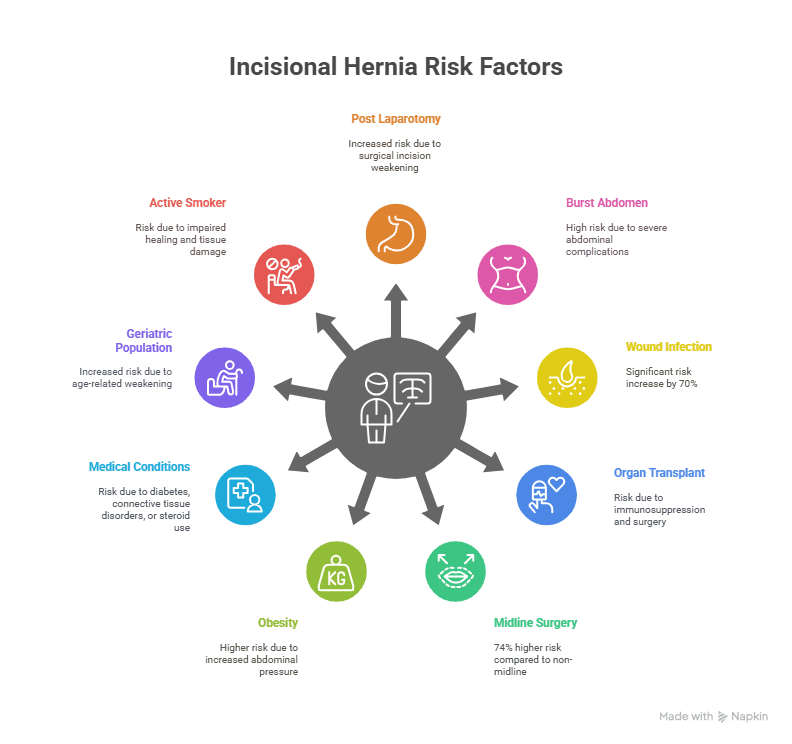
• Post Laparotomy
• Sequel of complications like burst abdomen
• Post-operative wound infection (This increases incisional hernia risk by 70%)
• Post liver or kidney transplant
• Midline bowel surgery or gynae surgery (There is a 74% risk increase compared to non-midline)
• BMI >25 Obese patients are more likely to develop an incisional hernia
• Diabetes Mellitus, Connective Tissue Disorders, or Steroid Use
• Geriatric Population
• Active Smoker
Treatment of Complex Hernia:
The treatment of complex hernias is an outstanding example for the so-called tailored approach in hernia surgery. Complex hernias are surgical challenges and their treatment requires the entire spectrum of techniques and equipment.
The optimal technique for repair varies depending on the exact situation including nutritional status, acute physiology, and the presence of contamination, amongst other factors.
Advanced surgical techniques of Complex Hernia Repair:
There are several cases where a simple conventional technique is not a viable option. To attempt an incisional hernia repair in such cases several advanced techniques and approaches have been advised.
The most common of these is a component separation technique (CST). With time this has been advanced to component separation technique with Transversus Abdominis Muscle Release. This is the most advanced technology that offers several advantages over conventional techniques in the management of complex incisional hernias.
Component separation is an abdominal wall reconstructive technique that strategically divides the rectus and lateral abdominal wall musculofascial layers in order to achieve tension-free midline fascial approximation.
Depending on the muscle(s) divided, the techniques of component separation can be broadly categorized into :
Anterior Component Separation
Posterior Component Separation
Posterior Component Separation techniques:
The Rives-Stoppa retro rectus dissection
Transversus abdominis release (TAR)
Some other techniques are:
e-TEP (Extended totally extraperitoneal repair)
TARM (Trans-Abdominal Retro muscular)
TAPP (Transabdominal pre‐peritoneal)
TAP (Totally extraperitoneal)
The concept of component separation technique (CST) for the treatment of very large primary and incisional abdominal wall hernias was developed because the traditional suture and mesh techniques without relaxing the musculofascial flaps lead to unfavourable results.
The Rives-Stoppa
Complex hernias especially recurrent have been managed by the Rives-Stoppa technique which is an established suture-less, tension-free, and absolute method of treatment with minimal recurrence rates.
The Rives-Stoppa repair for complex incisional hernias confers the benefits of prosthetic repair and lower recurrence rates, but decreases certain complications (fistula formation, adhesions, skin erosion, and seroma/abscess formation) by preventing direct mesh contact with the bowel.
The steps of a posterior component separation with mesh placement (Rives Stoppa) are as follows:
Incision and access to the abdominal cavity
Hernia sac dissection and excision
Posterior rectus sheath dissection and closure
Mesh placement
Drain placement
Anterior rectus sheath closure
Skin closure
TAR (Transversus abdominis release)
Transversus Abdominis Release (TAR) is a newly developed technique used in abdominal wall reconstruction that delivers a lasting solution to various complex incisional hernias. TAR is a novel technique of abdominal wall reconstruction which is a modification of a posterior component separation for the repair of complex incisional hernia. It is the only technique that treats complicated incisional hernias at their source.
Novitsky et al. 2012, presented a novel technique that modified the traditional surgical approach (Usually the Rives-Stoppa procedure) for patients with important abdominal wall defects. As a result, the Transversus abdominis muscle release (TAR) was proposed, showing good results in terms of recurrence, and postoperative and intraoperative complications.
TAR technique is based on the principal goals of an abdominal wall reconstruction: restoration of abdominal wall functionality preserving autologous tissue, and reinforcement by a durable mesh with less proportion of complications.
The procedure takes about three hours and the patient usually stays in the hospital for a day or two.
Studies show that 5% of patients treated with TAR have a recurrence, a huge improvement over those treated with open surgery. In a review by Pauli et al., the outcome for TAR showed a wound complication rate of 3.4%–31% and a recurrence rate of 1.1%–7.3%.
Indications of TAR:
TAR is most suited for high-risk patients, such as the morbidly obese. Historically, such patients were told to lose weight to reduce the risk of recurrence, a goal many never reached, often because they wound up in the ER with a strangulated bowel before they could lose the weight. This predicament led to the development of the new technique.
Other factors that indicate TAR as noble procedure:
Diabetes, whose accompanying microvascular problems, and effect on the blood supply interfere with the healing of the abdominal wall
Rectus diastasis, a usually congenital but sometimes acquired issue involving the separation of the six-pack muscle
Connective tissue diseases
Previous hernia repair by open surgery
Types of Hernia where Transversus Abdominis Release (TAR) can provide better outcomes are:
Large and complex ventral hernias
Subxiphoid hernias
Parastomal hernia
Flank hernias
Suprapubic hernia
Recurrent hernias
Advantages of the TAR procedure:
The use of the Transverse Abdominis Release (TAR) technique has demonstrated several advantages over traditional techniques when addressing complex abdominal deficiencies.
TAR avoids large skin flaps with damage to perforator vessels, thus reducing the risk of skin necrosis, SSOs, and SSIs
TAR allows the closure of abdominal wall defects of up to 20 cm in width
TAR allows the implantation of very large uncoated standard alloplastic meshes in the most suitable retro muscular sublay plane.
In most TAR cases, no mesh fixation is necessary.
According to a recent systematic review, the SSO rates after open anterior and open TAR are comparable, but the recurrence rate after open anterior Component Separation Technique is higher compared to that of open TAR
Posterior component separation with retro rectus mesh placement offers the advantages of low recurrence rates, low rates of wound complications such as seroma or infection, and excellent incorporation of inexpensive, uncoated mesh into the abdominal wall.
The different ways in which the TAR procedure can be done:
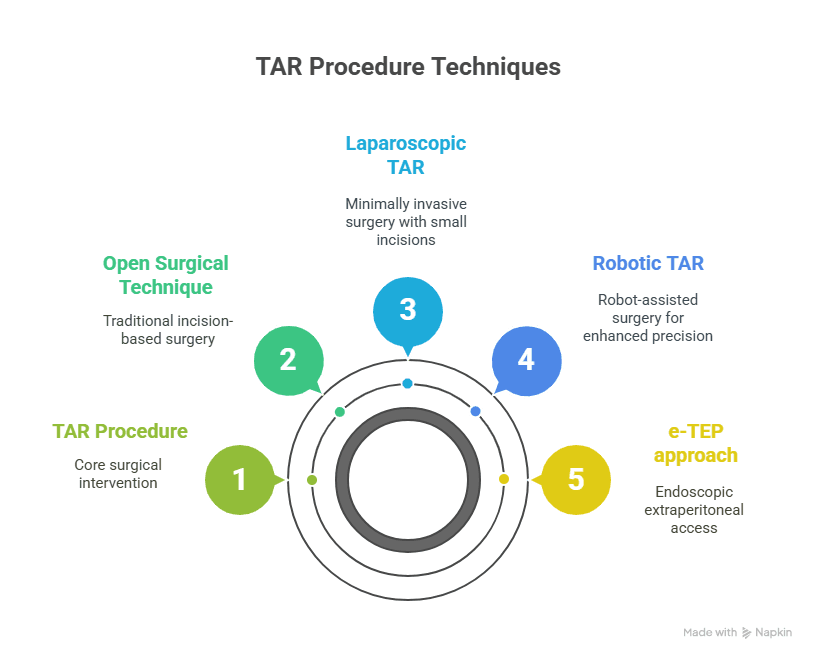
Open Surgical Technique
Laparoscopic TAR
Robotic TAR
e-TEP approach: e-TEP TAR
Unilateral TAR: either Open, Laparoscopic, e-TEP, or Robotic
Precautions after TAR Surgery:
Avoid heavy lifting, strenuous exercise, or any activity that strains the abdomen
Stop smoking if applicable, as this can slow healing
Manage excess weight, as this can help reduce pressure on the abdominal wall
Make sure to manage any existing medical conditions, such as diabetes.
e-TEP (Extended totally extraperitoneal repair)
The enhanced view totally extraperitoneal (e-TEP) technique which was described mainly for laparoscopic inguinal hernia repair is now a platform for the repair of ventral and incisional hernias as well. eTEP is an attractive option for selected cases because of improved outcome.
Features of eTEP technique are:
1. Fast and easy creation of the extraperitoneal space.
2. A large surgical field.
3. A flexible port setup adaptable to many clinical situations.
4. Unencumbered parietalization of the cord structures (proximal dissection of the sac and
peritoneum).
5. Easier management of the distal sac in cases of large inguinoscrotal hernias.
6. Improved tolerance of pneumoperitoneum, which is a common complication.
Indications for eTEP
We use the eTEP technique to repair most cases of inguinal hernias; however, there are cases for which eTEP is especially useful.
1. eTEP is easier to master for surgeons new to the technique.
2. Obese or post-bariatric patients: eTEP allows the surgeon to avoid the difficulties caused by the pannus; in addition, the subcutaneous tissue is thinner and higher in the abdomen.
3. When the distance between the umbilicus and pubic tubercle is short.
4. In patients with previous pelvic surgeries.
5. Wide variety of indications: with experience, surgeons can expand the indications for eTEP for inguinal hernia repair to cases of large inguinoscrotal, sliding, or incarcerated hernias. This may require a combination with a 5 mm laparoscopic intraperitoneal approach to verify the viability of the intestine or assist in reducing the incarcerated content.
Laparoscopic Trans-Abdominal Retromuscular (TARM)
TARM repair, introduced by Masurkar, is a transperitoneal low-cost procedure that could be performed with conventional instruments with an ergonomic triangulation of the ports, making intracorporeal suturing more convenient.
TARM reduces the probability of bowel injury. The working space is wider than the retro rectus space, allowing better vision, dissection, and suturing. However, this technique required an additional set of ports to create the same space on the opposite side.
A horizontal closure of the posterior rectus sheath is routinely performed in TARM, which would decrease the chances of complication. This may be attributed to the horizontal orientation of aponeurotic fibers in the posterior rectus sheath, which is thus better approximated horizontally than vertically.
For irreducible ventral hernia, TARM appeared to be safer than eTEP as the reduction of hernia contents was under vision, which was further aided by ergonomic port placement and wider working space, allowing ease in adhesiolysis.
Laparoscopic TARM was found to be effective for repairing small- and medium-sized irreducible ventral hernias. Sublay mesh placement avoided mesh–bowel contact.
Myo-fascial medicalization for tension-free closure, if needed, could be achieved via posterior component separation-transversus abdominis release with the same port
The larger working space and clear anatomy provide easy understanding and reproducibility.
Intraperitoneal composite meshes, balloon dissectors, and robotic arms were not needed. Further cost reduction could be achieved by using electrosurgical dissection instead of a harmonic scalpel.
Loss of Domain:
Incisional hernia treatment is challenging for surgeons, especially when there is a loss of domain. This ‘‘loss of domain’’ means that the herniated viscera of the abdominal content inhabit, in a permanent way, the hernia sac, which behaves like a second abdominal cavity. Restoring the hernia sac contents to the abdominal cavity may lead to respiratory and circulatory disturbances. It can also result in abdominal compartment syndrome (ACS), which occurs when the intra-abdominal pressure (IAP) rises faster than physiological adaptations and can be fatal in severe situations
The relationship between the volume of the hernia sac versus the volume of the abdominal cavity is the best criterion for defining whether there is a loss of domain (LOD).
LOD is defined when the volume of the sac/hernia content is greater than 25% of the volume of the abdominal cavity.
This fundamental information allows the surgeon to consider that:
There may not be enough space to reduce all herniated contents into the abdominal cavity and still achieve a complete primary fascial closure.
The significant increase in intra-abdominal pressure, due to the reduction of a large volume of content in the abdominal cavity, can cause important ventilatory restriction due to the upward compression of the diaphragm.
For tomographic assessment of the risk of LOD in bulky hernias, we used the method described by Tanaka et al because it is simple to understand
A- The largest measurement of each axis should be used, even in different tomographic sections to calculate the volume of the hernia sac, as well as the volume of the abdominal cavity.
B- To determine the abdominal volume cavity (AVC), some reference points must be used:
The measurement of the anteroposterior axis of the abdominal cavity is determined by the line that joins the muscle groups of the healthy (anterior) wall and the line that passes through the transverse processes of the vertebra (posterior).
The CC distance is made between the first cut showing the diaphragm and the last cut showing the tailbone. The transverse distance (T) through the parietal peritoneum on each side of the abdominal cavity.
C- To determine the hernia sac volume (HSV),
Measurement of the limits of the parietal peritoneum of the hernia sac for the CC and T axes. For the AP axis, the distance between the anterior parietal sac peritoneum hernia to a line joins the muscle groups of the healthy wall (posterior limit).
RV = HSV/ AVC
if >25% = loss of domain
Post-operative care:
The post-surgery patient is transferred to the recovery area. The anesthetist and nursing staff closely monitor the patient till the patient’s vital and pain become stable.
Once the patient becomes stable, the patient can be shifted to the ward. In most of the cases, patients are given sips of water and if tolerated well, the patient can also be given water.
IV lines stay in place until the patient can tolerate adequate liquids. Once the patients pass flatus, patients are allowed to take soft food, followed by a normal diet
Straining should be avoided due to constipation.
To avoid deep vein thrombosis (DVT) patients are counseled to avoid dehydration, ambulation, and stockings
Recovery After Hernia Surgery:
Recovery after hernia surgery is a critical phase that determines the long-term success and patient comfort following the procedure. Whether you've undergone open hernia repair or laparoscopic hernia surgery in Delhi, understanding the recovery process helps minimize complications and promotes faster healing.
Key Recovery Guidelines:
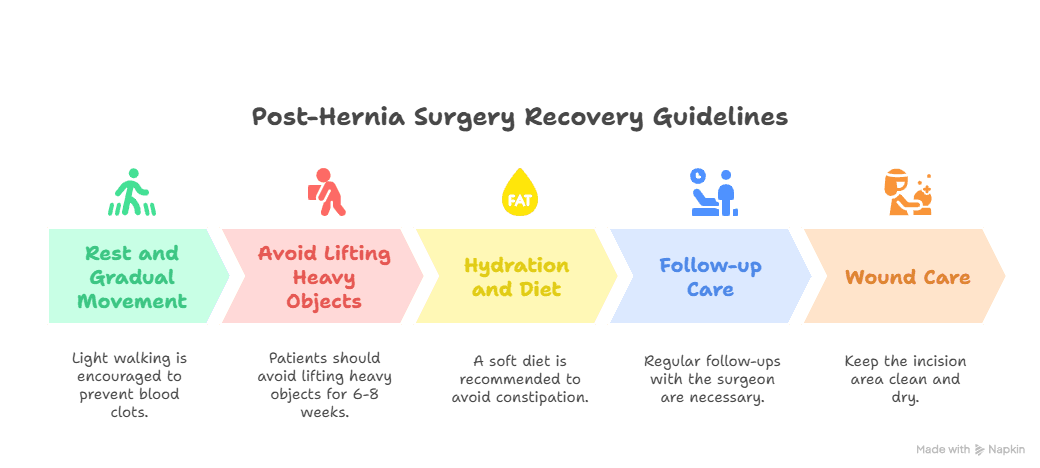
Rest and gradual movement: Light walking is encouraged within 24 hours to prevent blood clots.
Avoid lifting heavy objects: Patients should avoid lifting anything heavy or straining for at least 6–8 weeks post-surgery.
Hydration and diet: A soft diet is recommended initially to avoid constipation and pressure on the surgical site.
Follow-up care: Regular follow-ups with your surgeon, such as the best doctor for hernia surgery in Delhi, ensure proper healing and check for signs of recurrence or infection.
Wound care: Keep the incision area clean and dry. Watch for signs of redness, swelling, or unusual discharge.
Those who undergo hernia surgery in Apollo Delhi benefit from structured post-operative care that includes detailed discharge instructions, pain management, and diet counseling. These are important in ensuring patients return to work and daily life with minimal downtime.
Why Dr. Aloy Mukherjee is the Best Hernia Surgeon in Delhi?
Choosing Dr. Aloy Mukherjee for hernia surgery in Delhi is a decision that brings confidence and peace of mind to patients facing the need for this critical procedure. Dr. Mukherjee is a highly respected surgeon with extensive experience in performing complex hernia surgeries. His expertise is complemented by his use of the latest surgical techniques and state-of-the-art equipment, ensuring that patients receive the most advanced care available.
Dr. Mukherjee takes a patient-centered approach to hernia surgery, which begins with a thorough consultation to discuss each patient’s specific condition and the best surgical options available for them. He is known for his compassionate care and the personalized attention he gives to every patient, addressing all their concerns and ensuring they understand every step of the process.
Our Happy Patients
Mrs. Abida Khatun suffered from a Hernia, for which she underwent a successful surgery under the special care of Dr. Aloy J Mukherjee, Sr. Consultant - Bariatrics, Laparoscopic and General Surgeon at Indraprastha Apollo Hospitals, New Delhi.
Watch Mrs. Abida Khatun sharing her experience of safe and secure surgery at Indraprastha Apollo Hospitals, Delhi.
Frequently Asked Questions
Q1. What is hernia surgery?
Hernia surgery is a procedure to repair a hernia, which occurs when an internal organ or tissue bulges through a weak spot in the muscle. It involves either open surgery or laparoscopic (minimally invasive) surgery.
Q2. Who needs hernia surgery?
Hernia Surgery is recommended for individuals experiencing pain, discomfort, or complications from a hernia that cannot be managed with non-surgical treatments..
Q3. What types of hernia surgeries are available?
There are two main types of hernia surgery: open hernia repair, where a single large incision is made, and laparoscopic hernia repair, which uses several small incisions and a camera.
Q4. What is the recovery time for hernia surgery?
Recovery time for Hernia Surgery varies; most patients recover from laparoscopic surgery within 1-2 weeks, while open surgery may take 4-6 weeks for full recovery.
Q5. What are the risks of hernia surgery?
Risks of hernia surgery include infection, bleeding, recurrence of the hernia, and damage to surrounding tissues. However, these risks are generally low, especially with experienced surgeons.
Q6. How do I prepare for hernia surgery?
Preparation for Hernia Surgery involves fasting before the procedure, stopping certain medications, and undergoing pre-surgical tests as advised by your surgeon.
Q7. What should I expect after hernia surgery?
After hernia surgery, you can expect some pain and discomfort, which will be managed with medication. Most patients can return to normal activities within a few weeks.
Q8. Are there any dietary restrictions after hernia surgery?
Initially, after hernia surgery, it's advisable to follow a light diet to avoid straining the repaired area. Gradually, you can return to a normal diet based on your body's tolerance.
Q9. How much does hernia surgery cost?
The cost of Hernia Surgery in Delhi varies depending on the type of surgery, hospital, and surgeon's fees. It's best to consult with your healthcare provider for an accurate estimate.
Q10. Can a hernia recur after surgery?
While hernia surgery aims to repair the hernia, there is a small risk of recurrence. Following post-surgery care instructions and avoiding heavy lifting can help minimize this risk.