Hernia Surgery in Delhi: Dr. Aloy Mukherjee
Minimally invasive solutions for hernias, offering faster recovery, less pain, and minimal scarring.
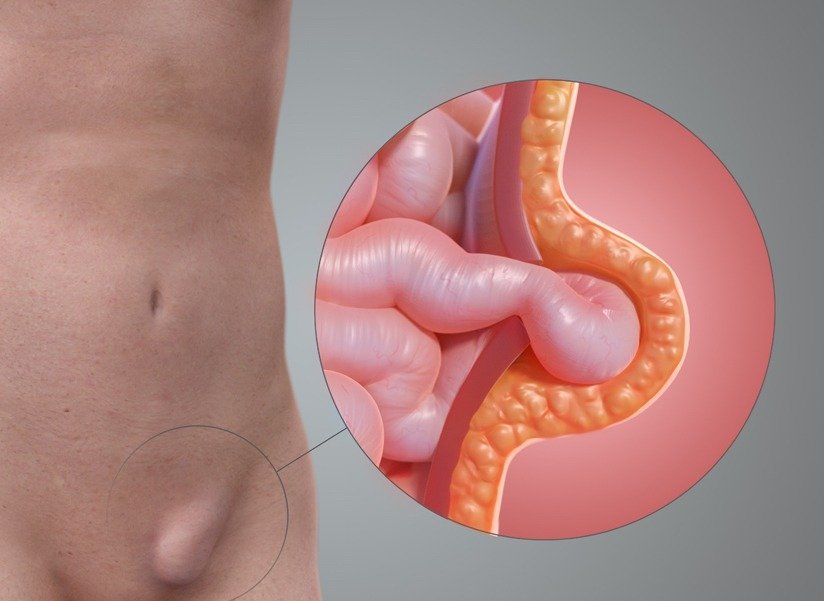
Understanding Hernia
Hernia surgery is a procedure performed to repair a hernia, which occurs when an internal organ pushes through a weak spot in the muscle or tissue. This condition can cause pain, discomfort, and visible swelling, especially during physical activity. Hernia surgery helps in repositioning the organ and strengthening the weakened area using advanced techniques. With modern advancements, Hernia Surgery in Delhi is now safer, more effective, and minimally invasive.
Common Causes & Risk Factors
Several factors contribute to this condition. Understanding these risks can aid in prevention and management.
Weak Abdominal Muscles
A hernia often develops due to weakness in the abdominal wall, which may be present from birth or develop over time due to aging or previous surgeries.
Heavy Lifting and Physical Strain
Frequent heavy lifting or intense physical activity increases pressure on the abdominal muscles, making them more prone to developing a hernia.
Chronic Cough or Constipation
Conditions like persistent coughing or long-term constipation can strain the abdominal area, increasing the risk of hernia formation.
Obesity and Lifestyle Factors
Excess body weight puts added pressure on the abdomen, while lack of exercise and poor lifestyle habits can weaken muscles and raise the chances of a hernia.
Symptoms of Hernia
Visible Bulge or Swelling
One of the most common signs of a hernia is a noticeable bulge or lump in the affected area, especially when standing, coughing, or straining.
Pain or Discomfort
Patients may experience pain or a dragging sensation at the site of the hernia, which often worsens during physical activity or lifting.
Heaviness or Pressure
A feeling of heaviness, pressure, or weakness in the abdomen or groin is a common symptom, particularly after prolonged standing or exertion.
Burning or Aching Sensation
Some individuals may feel a burning or aching sensation around the bulge, indicating irritation of surrounding tissues.
Diagnosis Process
To definitively diagnose Hernias and rule out other causes, our clinic utilizes comprehensive testing.
Physical Examination
The doctor begins with a detailed physical examination to check for visible bulges or swelling. Patients may be asked to cough or strain to make the hernia more noticeable.
Imaging Tests
In some cases, imaging tests such as ultrasound, CT scan, or MRI are recommended to confirm the diagnosis and assess the size and type of hernia.
Medical History Evaluation
The doctor reviews the patient�s medical history, symptoms, and lifestyle factors to determine the severity of the condition and plan the most suitable treatment.
Treatment Options for Hernia
Robotic Hernia Repair
Robotic hernia repair is an advanced, minimally invasive technique that uses robotic-assisted technology for greater precision and control. This approach allows the surgeon to perform complex repairs with smaller incisions, reduced pain, and minimal scarring.
Laparoscopic Hernia Repair
Laparoscopic hernia repair is a widely used minimally invasive procedure performed using small incisions and a camera-guided system. It provides a clear view of the affected area, allowing accurate repair of the hernia with less tissue damage.

Experience
Why Dr. Aloy Mukherjee is the Best Hernia Surgeon in Delhi?
Dr. Aloy Mukherjee is highly regarded for his expertise in treating all types of hernias using advanced and minimally invasive techniques. With years of surgical experience and a strong focus on precision, he ensures effective treatment with minimal discomfort and faster recovery. His ability to handle both simple and complex cases with confidence has earned him a reputation as a trusted specialist. This excellence makes him a preferred choice for patients seeking reliable hernia care.
What truly sets Dr. Aloy Mukherjee apart is his patient-first approach and commitment to delivering personalized treatment plans. He carefully evaluates each case and recommends the most suitable surgical method, whether laparoscopic or robotic. His use of modern technology, combined with compassionate care, ensures safe procedures and long-term results. Known for consistent success rates and patient satisfaction, he is widely recognized as a leading hernia surgeon in Delhi.
Read MorePatient Testimonials
Frequently Asked Questions
What is a hernia?
A hernia occurs when an internal organ pushes through a weak spot in the muscle or tissue, often causing a visible bulge and discomfort.
Is hernia surgery the only treatment?
Yes, surgery is the only permanent solution for a hernia. Non-surgical methods may provide temporary relief but do not fix the underlying issue.
Is hernia surgery painful?
Modern techniques like laparoscopic and robotic surgery involve minimal pain. Most patients experience mild discomfort that improves quickly during recovery.
How long does it take to recover after surgery?
Recovery time depends on the type of surgery, but most patients can return to normal activities within a few days to a couple of weeks.
Who is the top hernia surgeon in Delhi?
Dr. Aloy Mukherjee is considered one of the top hernia surgeons in Delhi, known for his expertise and successful treatment outcomes.
Can a hernia come back after surgery?
While recurrence is rare, it can happen in some cases. Following post-surgery guidelines and maintaining a healthy lifestyle can help reduce the risk.
Hernia Surgery Near You
Dr. Aloy Mukherjee provides expert hernia surgery for patients across Delhi NCR and nearby cities. Find hernia surgery services near your location.
Book Your Appointment
Get expert surgical care. Fill out the form below and we'll get back to you promptly.
Visit Us
Address
2nd floor, Indraprastha Apollo Hospital, Room No. 1265,
Gate No. 10, Jasola Vihar, New Delhi, Delhi 110076
Contact Information
Phone
+91 9810532834
contact@draloymukherjee.com
Timings
Monday- Saturday: 08:00 AM- 08:00 PM
Sunday: Closed
Emergency: 24/7 Available